
Table of Contents
- • What Is Pulp Capping?
- • Types of Pulp Capping: Direct vs Indirect
- • How Is Pulp Capping Performed?
- • What Materials Are Used in Dental Pulp Capping?
- • Pulp Capping vs Root Canal: Key Differences
- • How Painful Is a Pulp Cap?
- • How Long Can Pulp Capping Last?
- • Is Pulp Capping the Same as a Filling?
- • Pulp Capping Cost
- • Frequently Asked Questions
What Is Pulp Capping?
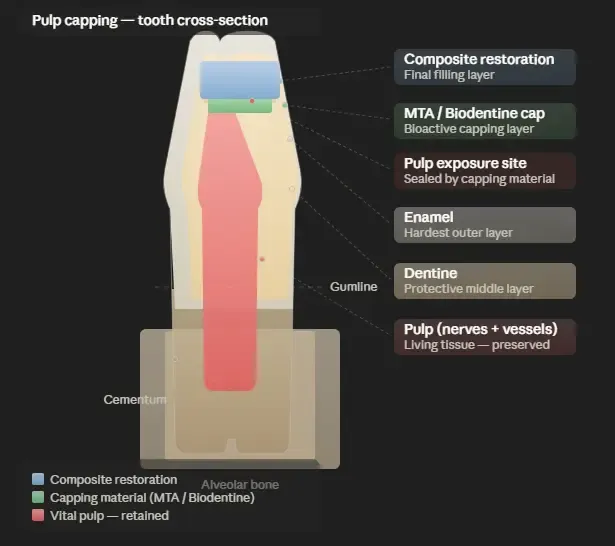
Pulp capping is a conservative dental procedure that places a medicated dressing over exposed or nearly exposed dental pulp to preserve its vitality and prevent the need for root canal treatment.
The dental pulp is the soft, living tissue at the centre of a tooth, containing nerves, blood vessels, and connective tissue that sustain the tooth through its lifetime. When deep decay, a crack, or accidental cavity preparation brings this tissue close to or into contact with the oral environment, bacteria can enter and cause irreversible inflammation. Pulp capping interrupts this process at an early stage by sealing the site with a biocompatible material that stimulates the formation of new protective dentine while keeping the pulp alive.
The procedure sits within the broader field of vital pulp therapy, which aims to maintain or restore pulp health rather than remove the pulp entirely. Research published in dental literature confirms that preserving pulp tissue is preferable to root canal treatment where possible, because an intact pulp retains its developmental, defensive, and sensory functions, and the tooth avoids the structural weakening that typically follows pulpectomy.
When Is Pulp Capping Indicated?
Pulp capping is appropriate when the pulp is either inadvertently exposed during cavity preparation or is in very close proximity to the surface of a deep carious lesion, provided the pulp tissue itself shows no signs of irreversible inflammation or infection. The most favourable candidates are teeth diagnosed with reversible pulpitis, meaning they produce a response to cold or pressure that resolves within seconds rather than lingering for minutes.
Key indicators that pulp capping may be suitable include the absence of spontaneous pain prior to treatment, a controlled and minimal exposure site ideally less than one millimetre in diameter, no pus or discharge from the exposed pulp, and a radiograph showing no periapical bone changes. Age also plays a role: younger patients with open or recently closed root apices tend to achieve better outcomes because pulp tissue retains greater regenerative capacity.
When Is Pulp Capping Not Appropriate?
Pulp capping is contraindicated when the pulp shows signs of irreversible pulpitis or necrosis. Clinical signs that indicate pulp capping would be unlikely to succeed include spontaneous or prolonged throbbing pain, a fistula or sinus tract near the tooth, significant bleeding that cannot be controlled at the exposure site, radiographic evidence of widened periodontal ligament space, or a history of recurrent infection around the same tooth. In such cases, root canal treatment is the appropriate course of action.
Types of Pulp Capping: Direct vs Indirect
Pulp capping describes two distinct clinical techniques that differ in whether the pulp tissue has been physically exposed.
Direct Pulp Capping
Direct pulp capping is performed when the pulp has been mechanically or accidentally exposed during the removal of decay or cavity preparation. In this technique, the capping material is placed in direct contact with the exposed pulp tissue itself. The goal is to seal the opening, control any bleeding, and encourage the pulp to form a dentine bridge over the exposure site. Direct pulp capping is a single-stage procedure and is most predictable when the exposure is small, haemorrhage is minimal, and contamination has been kept to a minimum using a rubber dam.
Indirect Pulp Capping
Indirect pulp capping is used when deep decay comes extremely close to the pulp without actually exposing it. Instead of removing every trace of softened dentine, which would risk perforation, the dentist leaves a thin layer of affected dentine in place and covers it with a biocompatible capping material. This approach relies on the natural ability of the pulp to form reactionary dentine beneath the capping material, progressively remineralising the area. In some protocols, the tooth is temporarily restored and reviewed after three to six months before a second appointment removes the temporary restoration and assesses healing. Indirect pulp capping may also be completed as a one-visit procedure when the residual dentine layer is judged thick enough to provide adequate protection.
How Is Pulp Capping Performed?
The pulp capping procedure follows a well-defined clinical sequence that typically requires one or two appointments depending on the technique used.
Preparation and Isolation
The first step is administering a local anaesthetic to ensure the patient is fully comfortable throughout treatment. Rubber dam isolation is then applied to the tooth, creating a dry, bacteria-free operating field. This step is critical: contamination from saliva during pulp capping dramatically reduces the likelihood of success. The dentist then removes decay using rotary instruments or hand excavators, progressing carefully as the preparation approaches the pulp to avoid an uncontrolled perforation.
Exposure Management and Haemostasis
If direct pulp capping is being performed, the exposure site is gently irrigated with sodium hypochlorite or sterile saline to disinfect the area and assess bleeding. A dry cotton pellet or a haemostatic agent is applied for one to two minutes to control haemorrhage. Persistent, uncontrollable bleeding at this stage is considered a warning sign of deeper pulpal inflammation, and the dentist may instead proceed with a partial pulpotomy or root canal treatment. For indirect pulp capping, no exposure exists, and the dentist simply ensures the remaining dentine layer is clean and dry before placing the capping material.
Placement of the Capping Material
Once the field is prepared, the capping material is placed over the exposure site (for direct pulp capping) or over the remaining dentine (for indirect pulp capping). Materials such as mineral trioxide aggregate (MTA) or calcium silicate cements are mixed and applied in a thin layer covering the entire exposure and the immediately surrounding dentine. The material is then left to begin setting. A protective base of glass ionomer cement or composite may be placed over the capping agent to provide an additional seal before the final restoration is applied.
Restoration and Follow-up
The tooth is restored in the same visit with composite resin, or provisionally sealed if a two-visit protocol is being followed. An adequate coronal seal is considered essential to the long-term success of pulp capping, because the capping material alone will not prevent bacterial microleakage from a poorly fitted restoration. At follow-up appointments, the dentist assesses pulp vitality through cold testing and radiographic examination, checking for dentin bridge formation, continued normal root development in younger patients, and the absence of pathological signs.
What Materials Are Used in Dental Pulp Capping?
Pulp capping materials are biocompatible agents applied over dental pulp or near-pulp dentine to stimulate healing and dentine bridge formation.
The choice of material has a direct bearing on clinical outcomes. Research shows that hydraulic calcium silicate cements currently produce the most predictable results, while calcium hydroxide, once the gold standard, has largely been replaced in contemporary practice due to its tendency to produce tunnel defects in the dentine bridge it stimulates.
Mineral Trioxide Aggregate (MTA)
Mineral trioxide aggregate is a calcium silicate-based cement developed in the early 1990s and has become the reference material for vital pulp therapy in permanent teeth. MTA maintains a high alkaline pH over the long term, which creates an inhospitable environment for bacteria while stimulating the formation of a continuous dentine bridge at the exposure site. Clinical studies following MTA-treated teeth for up to ten years report success rates exceeding 90% in appropriately selected cases. MTA is biocompatible, resistant to bacterial microleakage, and capable of setting in the presence of moisture, which is clinically advantageous given that pulp tissue is inherently moist. Its principal drawbacks are a relatively long setting time and the potential for tooth discolouration with grey formulations. White MTA is preferred in anterior teeth for this reason.
Biodentine (Calcium Silicate Cement)
Biodentine is a tricalcium silicate-based material introduced as a dentine substitute that can be used for both direct and indirect pulp capping. It offers similar biological properties to MTA, including the stimulation of reparative dentine formation and good biocompatibility, while addressing some of the handling limitations of conventional MTA. Biodentine sets in approximately twelve minutes, making it considerably faster than standard MTA, and its physical properties after setting closely resemble those of natural dentine. Clinical studies show success rates comparable to MTA at two to three years, with the advantage of superior handling characteristics that many clinicians find easier to manipulate in confined spaces.
Calcium Hydroxide
Calcium hydroxide was the dominant pulp capping material for most of the twentieth century and remains in use in many general practices today. Its antibacterial properties, derived from its high alkalinity, can suppress bacterial growth at the exposure site, and it is capable of stimulating reparative dentine formation. However, systematic reviews of long-term outcomes indicate progressively declining success rates compared to MTA and calcium silicate cements: success at four to five years falls to approximately 56% for calcium hydroxide versus approximately 81% for MTA. The dentine bridges formed over calcium hydroxide caps are also reported to contain tunnel defects more frequently, meaning pathways through which bacteria could eventually reach the pulp remain present. Calcium hydroxide continues to play a role in specific clinical situations, particularly in indirect pulp capping in primary teeth and in combination with other materials.
Glass Ionomer Cement and Resin-Based Adhesives
Glass ionomer cements release fluoride and bond to tooth structure, making them a useful secondary layer over calcium silicate materials in pulp capping restorations. They provide an effective coronal seal that protects the capping material below and reduce the risk of microleakage. Resin-based adhesive systems have also been studied as pulp capping agents, though their direct application on exposed pulp tissue is generally considered less favourable than calcium silicate materials due to potential cytotoxic effects of resin monomers on pulp cells.
Pulp Capping vs Root Canal: Key Differences
Pulp capping and root canal treatment address different stages of pulp disease and involve substantially different levels of clinical intervention.
Pulp capping is appropriate when the pulp is vital and shows at most reversible inflammation. The procedure preserves the living pulp tissue in its entirety and involves placing a capping material over the exposure site before sealing the tooth with a standard restoration. Because the pulp remains intact, the tooth retains its nerve supply, blood circulation, and natural capacity to respond to further stimuli. Teeth that have undergone successful pulp capping generally do not require crowns, though a full-coverage crown may still be recommended for heavily restored back teeth.
Root canal treatment, by contrast, is indicated when the pulp has become irreversibly inflamed or has begun to necrose. The entire pulp, including the tissue within the root canals, is removed and replaced with an inert filling material. The procedure requires multiple files, irrigation protocols, and canal-shaping steps that can take one to three appointments. Root canal-treated teeth lose their internal blood supply, which over time makes the dentine more brittle and increases the risk of fracture. This is why a crown is routinely recommended after root canal treatment, adding to the overall cost and time investment.
From a cost-effectiveness perspective, a study published in clinical dental literature found that pulp capping in children and adolescents with carious pulp exposures resulted in approximately 367 euros lower in total cumulative treatment costs over nine years compared with initial root canal treatment, including the cost of any subsequent retreatment needs.
Choosing Between Pulp Capping and Root Canal
The decision depends primarily on the clinical and radiographic diagnosis. A dentist who diagnoses reversible pulpitis with a small, clean exposure in a patient without spontaneous pain will consider pulp capping the conservative first choice. Where the diagnosis is irreversible pulpitis, pulp necrosis, or periapical pathology, root canal treatment is not optional and pulp capping would represent an inappropriate delay of necessary care.
How Painful Is a Pulp Cap?
Pulp capping, when performed correctly under local anaesthesia, is not a painful procedure, and post-operative sensitivity is typically mild and self-limiting.
During the Procedure
The treatment is carried out under local anaesthesia, which renders the area completely numb. Patients may feel pressure from instruments or vibration from the drill but should not experience pain. If any discomfort is felt during treatment, additional anaesthetic is applied. The use of rubber dam isolation, while not physically uncomfortable, helps maintain a controlled and clean field, which indirectly contributes to treatment success.
After the Procedure
Once the anaesthetic wears off, some sensitivity to cold temperatures or biting pressure is normal and expected in the days following pulp capping. This occurs because the pulp has been disturbed and may be mildly inflamed as a natural response to the procedure. Most patients report that any post-operative sensitivity resolves within one to two weeks. Over-the-counter analgesics such as ibuprofen are generally sufficient for managing any discomfort during this period.
When Sensitivity Does Not Resolve
If sensitivity to cold or pressure persists beyond two to three weeks, increases in intensity, or is joined by spontaneous or throbbing pain, these are signals that the pulp may not have healed as expected. The patient should return to the clinic for re-evaluation. In a proportion of cases, even correctly performed pulp capping with contemporary materials does not prevent eventual pulp degeneration, particularly in teeth with larger exposures or pre-existing pulpal inflammation that was more advanced than the pre-operative diagnosis indicated. In such situations, root canal treatment is the appropriate next step.
How Long Can Pulp Capping Last?
The longevity of a pulp cap depends on the material used, the accuracy of the initial diagnosis, the quality of the coronal restoration, and the patient's oral hygiene over time.
Success Rates by Material
Published clinical evidence provides the clearest picture of durability when broken down by the capping material used. For mineral trioxide aggregate (MTA), reported success rates from peer-reviewed studies are approximately 91% at six months, 86% at one year, 84% at two to three years, and 81% at four to five years. Biodentine shows comparable early results with approximately 91% success at six months and 86% at one year, with longer-term data still accumulating. Calcium hydroxide demonstrates declining success over time, with rates of approximately 74% at six months, 65% at one year, 59% at two to three years, and 56% at four to five years.
Factors That Influence Longevity
The integrity of the final restoration placed over the capping material is one of the most significant determinants of long-term success. A failed or leaking filling allows bacteria to re-enter the pulp chamber and re-infect the capped site even if the original capping material performed well. Regular dental check-ups allow early identification of restoration breakdown before it compromises the pulp cap below. Patient age also matters: younger patients, particularly those in whom root formation was still incomplete at the time of treatment, tend to achieve more durable results because of the higher regenerative capacity of the pulp in developing teeth.
Is Pulp Capping the Same as a Filling?
Pulp capping and a dental filling are distinct procedures that serve different purposes, although a filling is typically placed over the capping material as the final step of treatment.
A dental filling addresses a cavity by removing decay and replacing lost tooth structure with a restorative material such as composite resin or amalgam. The filling itself makes no therapeutic contact with the pulp and does not stimulate dentine formation. It is a straightforward restorative procedure suitable for cavities of moderate depth.
Pulp capping is an additional step performed before a filling when the depth of decay or an accidental exposure brings the pulp into clinical focus. The capping material applied directly to the pulp or near-pulp dentine is a bioactive agent designed to promote healing, form a protective dentine bridge, and maintain pulp vitality. Without this capping step, a standard filling placed over an exposed or nearly exposed pulp would not provide the biological stimulus needed for repair and would likely fail to prevent subsequent pulp necrosis.
In terms of what the patient experiences, both procedures involve local anaesthesia, cavity preparation, and the placement of a final restoration, which is why the two are sometimes confused. The key distinction lies in the layer of therapeutic material applied beneath the final filling in a pulp capping case. A filling without pulp capping is appropriate for shallower cavities. Pulp capping with an overlying filling is a more advanced, biologically oriented intervention reserved for deep cavities where pulp involvement is a clinical concern.
Pulp Capping Cost
The cost of pulp capping depends on the country of treatment, the complexity of the case, the material used, and whether the procedure is performed alongside a routine filling or requires a standalone appointment.
Pulp Capping Cost in Western Countries
In the United States, the ADA procedure code for direct pulp capping (D3110) is billed separately from the final restoration. Fees from published dental fee schedules place direct pulp capping in the range of approximately USD 75 to USD 200 for the cap itself, with the final composite restoration adding a further USD 150 to USD 400 depending on the tooth and number of surfaces involved. Patients who have undergone the procedure out of pocket in the US have reported total costs in the range of USD 300 to USD 500 when the cap and the filling are billed together. Root canal treatment in the US, by comparison, typically ranges from USD 700 to USD 1,500 for a posterior tooth, not including the cost of a crown.
In the UK, pulp capping within NHS dentistry may fall under Band 2 treatment, though private dentists charge variable rates typically between GBP 80 and GBP 250 for the capping procedure alone. When combined with a private composite filling, the total cost for the visit can reach GBP 300 to GBP 500.
Pulp Capping Cost in Turkey
Turkey has established itself as one of the leading destinations for dental tourism globally, with cost savings of up to 70% compared to Western European and North American prices for an equivalent standard of care and materials. Pulp capping in Turkey is generally priced between EUR 50 and EUR 150 for the procedure itself, with the total cost for the appointment including the final restoration remaining well below comparable treatment costs in the UK or US.
The cost advantage in Turkey arises from lower operating expenses, favourable currency exchange rates, and competitive pricing among a large number of accredited clinics, rather than any compromise in the quality of materials or clinical protocols. Turkish dental clinics treating international patients routinely use the same bioactive capping materials, including MTA and Biodentine, that are standard in Western European practice. All-inclusive dental tourism packages for more complex treatment plans, including pulp capping, associated restorations, and pre-treatment diagnostics, are also widely available and represent a significant reduction in overall expenditure for patients from the UK, Germany, and other Western European countries.
DentalAYS Turkey provides detailed cost information and personalised treatment quotes during a free online consultation, allowing international patients to understand the full scope of their treatment and associated costs before travelling.
Frequently Asked Questions
What Is Pulp Capping In Dentistry?
Pulp capping is a dental procedure in which a biocompatible material is placed over exposed or nearly exposed dental pulp to protect it from bacteria, promote healing, and preserve the vitality of the tooth. It is used as an alternative to root canal treatment in cases where the pulp is still healthy or only mildly inflamed.
How Is Pulp Capping Performed Step By Step?
The procedure begins with local anaesthesia and rubber dam isolation. The dentist removes decay carefully until the exposure site is reached, controls any bleeding with a haemostatic agent or saline irrigation, and then places a capping material such as MTA or Biodentine directly over the exposure or the thin remaining dentine layer. A protective base and final restoration are then applied over the capping material in the same visit.
Can Pulp Capping Fail, And What Happens If It Does?
Pulp capping can fail if the pulp inflammation was more advanced than the pre-operative diagnosis indicated, if the final restoration fails and allows bacterial recontamination, or if the exposure site was too large or too contaminated at the time of treatment. A failed pulp cap typically presents as persistent or worsening pain, sensitivity that does not resolve, or radiographic evidence of periapical change. If failure is confirmed, root canal treatment is the appropriate next step to preserve the tooth.
Is Pulp Capping Covered By Dental Insurance?
Coverage depends on the patient's specific insurance policy and country of treatment. In many cases, pulp capping as a separate procedure code may be covered under restorative or endodontic benefits, but patients are advised to confirm this with their insurer before treatment. In Turkey, the procedure is priced affordably enough that many international patients opt to self-pay and still achieve significant savings compared to insured treatment at home.
How Long After Pulp Capping Should I Wait Before Getting A Crown?
In most cases, a full-coverage crown is not required after pulp capping unless the tooth has already lost significant structural tooth structure from the original cavity. When a crown is indicated, most dentists recommend waiting two to four weeks after pulp capping to confirm that the pulp has responded well to treatment, there is no residual sensitivity, and the capping material has fully set. The follow-up radiograph at this appointment helps confirm that the procedure has been successful before proceeding to crown preparation.
This article is intended for informational purposes only. Patients should seek a professional clinical evaluation to determine the most appropriate treatment for their individual circumstances. DentalAYS Turkey offers free online consultations with experienced dental specialists for international patients.
