Table of Contents
- • Why Does Smoking Affect Dental Implant Success?
- • What Are the Success Rates for Smokers With Dental Implants?
- • Do You Have to Quit Smoking Before Getting Dental Implants?
- • Alternatives or Extra Precautions for Smokers
- • Frequently Asked Questions (FAQ)
Can Smokers Get Dental Implants? Risks and Success Rates
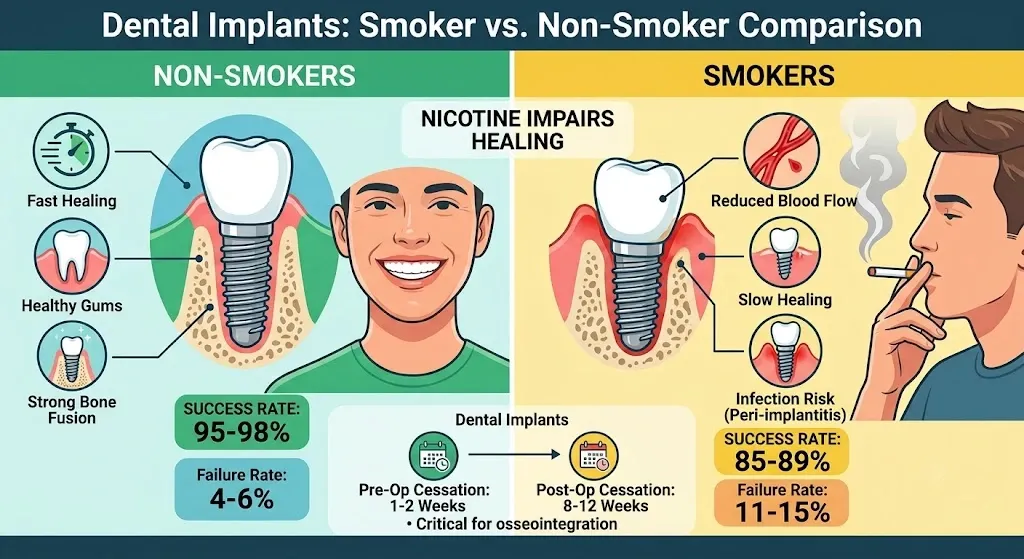
Yes, smokers can get dental implants, but success rates are lower than for non-smokers due to reduced blood flow and slower healing. Studies show implant failure rates of 11 to 15 percent in smokers compared to 4 to 6 percent in non-smokers. Quitting or pausing smoking around surgery significantly improves outcomes.
Key Highlights
- Implant failure rate: 11 to 15 percent in smokers vs 4 to 6 percent in non-smokers
- Pre-surgery smoking pause recommended: 1 to 2 weeks
- Post-surgery smoking pause recommended: 8 to 12 weeks, covering the osseointegration window
- Highest risk zone: upper jaw molar implants near the sinus
- Biggest controllable risk factor: smoking during the first 3 months of healing
Why Does Smoking Affect Dental Implant Success?
Smoking affects dental implant success by restricting blood flow to the gums and jawbone, which slows osseointegration, the process where the implant fuses with bone. Nicotine constricts blood vessels, carbon monoxide reduces oxygen delivery to healing tissue, and toxins in tobacco smoke impair white blood cell function needed to fight infection.
How Nicotine Delays Healing
Nicotine narrows blood vessels around the implant site for hours after each cigarette. This starves the surgical wound of oxygen and nutrients right when new bone cells need them most to attach to the implant surface.
Increased Risk of Peri-Implantitis
Smokers face a higher risk of peri-implantitis, a gum infection around the implant similar to periodontitis around natural teeth. Reduced immune response and poor circulation make it harder for the body to control bacterial buildup at the implant site.
Bone Density and Grafting Complications
Long-term smoking is linked to lower bone density in the jaw. Patients who need bone grafting before implant placement often see slower graft integration and higher graft failure rates if they continue smoking during recovery.
Our implant dentistry treatment page covers how we assess bone density and plan grafting during the consultation stage.
.
| Smoking Status | Average Failure Rate | Average Healing Time | Peri-Implantitis Risk |
|---|---|---|---|
| Non-smoker | 4 to 6 percent | 3 to 4 months | 5 to 10 percent |
| Light smoker (under 10/day) | 8 to 11 percent | 4 to 5 months | 15 to 20 percent |
| Heavy smoker (10+/day) | 15 to 20 percent | 5 to 7 months | 25 to 30 percent |
Figures are pooled averages from clinical studies on smoking and implant outcomes, intended as general guidance rather than individual prognosis.
What Are the Success Rates for Smokers With Dental Implants?
Dental implant success rates for smokers average 85 to 89 percent over 5 to 10 years, compared to 95 to 98 percent for non-smokers. Success rates improve substantially when patients stop smoking at least one week before surgery and avoid smoking for at least two to three months during healing.
Success Rates by Smoking Frequency
Heavy smokers, generally more than 10 cigarettes per day, show the steepest drop in success rates. Light or occasional smokers have outcomes closer to non-smokers, though still not equal.
Upper Jaw vs Lower Jaw Differences
Implants placed in the upper jaw, particularly the back molar area near the sinus, fail more often in smokers than implants in the lower jaw. The upper jaw bone is naturally softer and more dependent on good blood supply.
Factors that most influence the success rate for smokers:
- Cigarettes smoked per day
- Total years of smoking history
- Anatomical implant location (e.g., Upper vs. Lower jaw)
- Daily oral hygiene and maintenance routines
- Pre-existing bone density at the surgical site
Do You Have to Quit Smoking Before Getting Dental Implants?
You do not always have to quit smoking permanently before getting dental implants, but most clinics require a smoking pause of one to two weeks before surgery and at least eight to twelve weeks after, covering the critical osseointegration window. Complete cessation gives the best long-term results.
Recommended Pre-Surgery Smoking Pause
A one to two week break before surgery allows blood vessels to recover some normal function, improving initial healing conditions from the first day.
Recommended Post-Surgery Smoking Pause
The eight to twelve week window after placement covers the period when the implant is fusing with bone. Smoking during this stage is the single biggest controllable risk factor for early implant failure.
Are There Alternatives or Extra Precautions for Smokers Getting Implants?
Yes, smokers can improve implant outcomes through nicotine replacement therapy during the healing window, more frequent post-op checkups, antibacterial mouth rinses, and choosing implant systems or bone grafting techniques suited to lower bone density. Some clinics also recommend a longer healing period before loading the implant with a crown.
Nicotine Replacement During Recovery
Patches or gum are sometimes suggested instead of smoking during the critical healing weeks, since they avoid the vessel-constricting effect of inhaled smoke while managing cravings.
Extended Healing Protocols
Clinics may recommend waiting longer, sometimes 4 to 6 months instead of the standard 3 to 4, before attaching the final crown on a smoker's implant, giving bone extra time to integrate.
Choosing the Right Implant Material
Material choice also plays a role in long-term stability for smokers, since some materials bond with bone differently under reduced blood flow. Our comparison of zirconia vs titanium implants breaks down which option suits higher-risk cases.
FAQ
Can Heavy Smokers Still Get Dental Implants?
Yes, heavy smokers can still get dental implants, though failure risk is higher and dentists usually recommend cutting back significantly around the surgery date and healing period to protect the investment.
How Long Should I Stop Smoking Before Dental Implant Surgery?
Most dentists recommend stopping at least one to two weeks before surgery and staying smoke free for eight to twelve weeks afterward, since this covers the main bone fusion period.
Does Vaping Affect Dental Implants the Same Way as Smoking?
Vaping still delivers nicotine, which constricts blood vessels and can slow healing, so most clinics apply the same precautions to vapers as they do to cigarette smokers.
What Happens If I Smoke Right After Getting a Dental Implant?
Smoking soon after surgery reduces blood flow to the healing site, raises infection risk, and is one of the leading causes of early implant failure in the first few months.
Is Dental Implant Failure Reversible in Smokers?
A failed implant usually needs to be removed, the site allowed to heal, and a new implant placed later, often after further reducing smoking and sometimes after bone grafting to rebuild lost density. If you are researching clinics abroad, our guide on Turkey teeth explains how to vet clinic quality and avoid the risks tied to that reputation.
